Ask anyone building a healthcare navigation tool, a plan shopping experience, or a network analytics platform what keeps them up at night, and provider data accuracy will be near the top of the list. It's one of the most persistent, most consequential problems in health insurance technology — and it's one that Ideon has invested deeply in solving.
This post explains exactly how we approach provider data quality: the process, the checks, the people, and the standard we hold ourselves to every time data leaves our systems.
Why provider directory data goes stale — and why it matters
Provider data is not static. Physicians join and leave networks. Clinics change addresses. Group practices add and drop insurance contracts. Carriers update their directories continuously — but additions tend to outpace removals. The result is that stale records accumulate quietly over time, creating directories populated with providers who no longer accept a given plan, at addresses that are no longer correct, with specialties that no longer reflect where that provider practices.
For the platforms and tools that depend on this data, the downstream effects are significant. A care navigation tool that routes a member to an out-of-network provider — or worse, to an address that no longer exists — erodes trust and creates real financial harm. A plan shopping tool that tells a user their doctor is covered by a plan they ultimately enroll in, when they're actually out of network, is a serious compliance and experience failure. Network analytics platforms that start with inaccurate source data produce insights that mislead the carriers who rely on them.
Accurate provider network data is not a nice-to-have. It is foundational infrastructure.
How most approaches fall short
The most common approach in the industry is to ingest carrier-provided data files, normalize them into a consistent format, and pass them downstream. The problem is that this treats data accuracy as a carrier responsibility rather than a platform responsibility. Carrier data quality varies enormously — some carriers maintain highly structured, frequently updated directories; others rely on self-reported provider data that is months or years out of date.
Accepting carrier data at face value and passing it through creates a pipeline that is only as good as its weakest source. And because inaccuracies are often invisible until a member or a user surfaces them, they can persist in production systems for a long time before anyone notices.
Ideon takes a different approach. We treat data quality as an active responsibility — something we verify, validate, and stand behind at every step.
The Ideon data pipeline: quality built in at every stage
Every provider record that flows through Ideon's systems passes through a structured six-stage pipeline before it is ever delivered via the IdeonSelect provider network API. The stages are: Acquire → Validate → Map → Auto-QA → Human Review → Deliver
This is not a linear hand-off where each stage assumes the prior one was clean — it is a quality-gated process where data can only advance when the stage ahead of it is satisfied.
| Stage | What happens | Quality outcome |
|---|---|---|
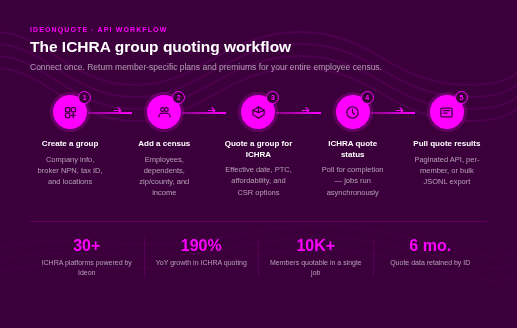
| 01 Acquire | Ingest provider network data from 300+ insurance carriers via structured feeds, file transfers, and direct API connections | Broad market coverage across all carrier types — not just carriers with clean data |
| 02 Validate | Check every record against structural and referential integrity rules — malformed records, missing required fields, invalid identifiers, out-of-range values | Records that fail validation are flagged and quarantined; they do not advance |
| 03 Map | Normalize carrier data into a single canonical schema — NPI numbers, taxonomy codes, specialty classifications, network participation flags, location data | Downstream platforms build against one predictable schema regardless of carrier origin; data that can't be reliably mapped is flagged rather than silently approximated |
| 04 Auto-QA | Run programmatic quality checks against every record and every run: sudden drops in network size, unexpected provider count changes by geography or specialty, duplicate records, address anomalies | Catches anomalies that pass structural validation but indicate a bad file — catches problems that are invisible at the record level but visible in aggregate |
| 05 Human Review | A human analyst reviews every single data run — investigating flagged issues, making judgment calls that rules alone can't encode, and signing off on the run | Zero unresolved flags before any data is promoted. Every run. No exceptions. |
| 06 Deliver | Only after clearing automated QA and human review is data promoted to the production API | Every API call returns data that has been through the complete pipeline |
Addressing the hardest data quality challenge: provider locations
Of all the fields in a provider directory, address data is among the most error-prone. Providers practice at multiple locations. Office addresses change. Suite numbers get formatted inconsistently across carrier files. And unlike a wrong phone number, a wrong address can send a member to a location where care is unavailable — or not covered.
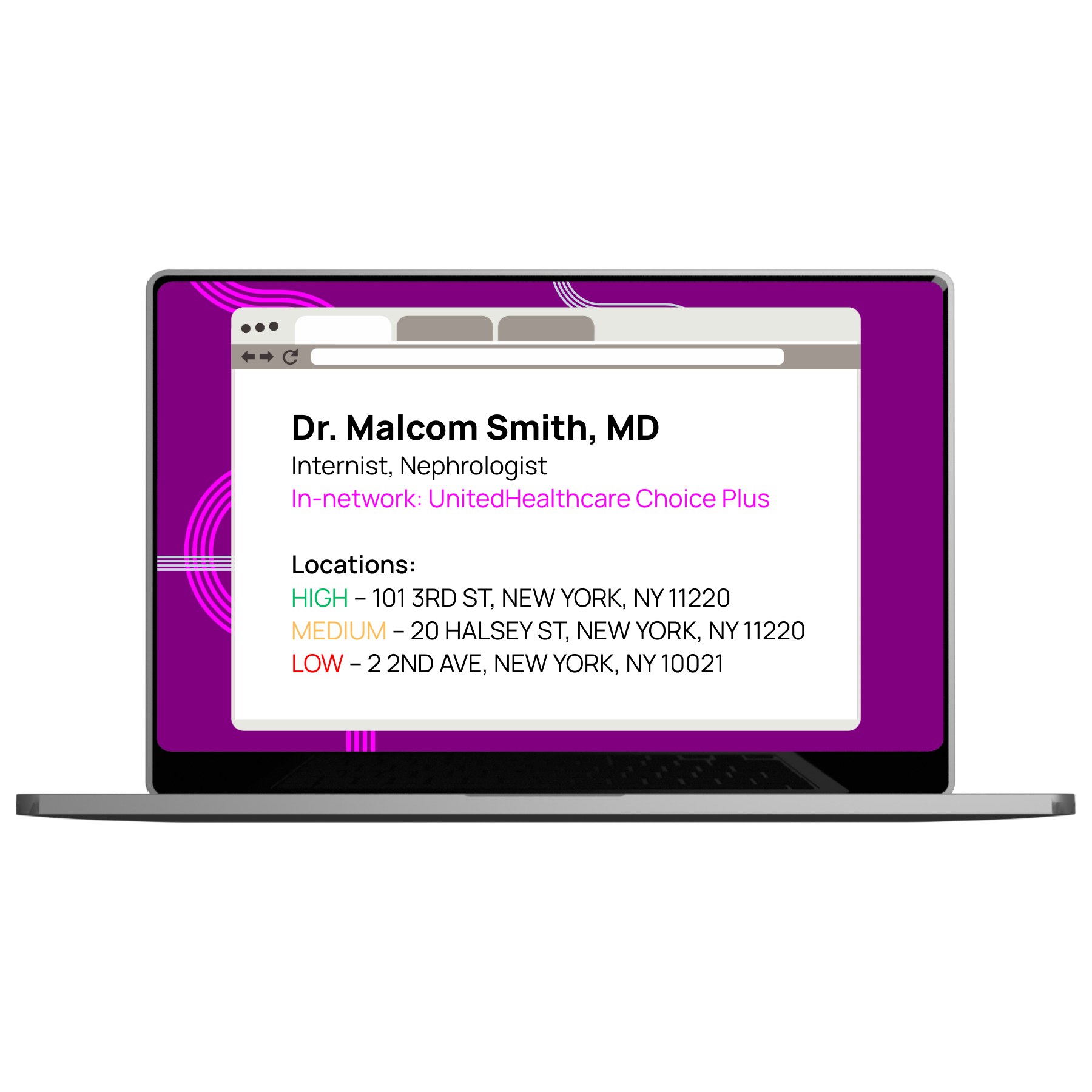
Ideon has developed an AI-driven Address Confidence Score that assigns a High, Medium, or Low confidence rating to every provider address in the IdeonSelect dataset. The model draws on multiple data sources and pattern analysis to assess address reliability — going beyond what any single carrier file can confirm.
| Confidence level | What it means | How platforms can use it |
|---|---|---|
| High | Address validated across multiple sources; high likelihood the provider practices here | Surface in search results with confidence; no additional member warnings needed |
| Medium | Address confirmed in some but not all sources; reasonable but not certain | Show in results; optionally surface a soft confirmation prompt before a member commits |
| Low | Address conflicts across sources or cannot be validated; higher risk of being incorrect | Filter from primary results, flag prominently, or prompt member verification before use |
This gives platforms built on IdeonSelect a new layer of control: the ability to filter or de-prioritize low-confidence addresses in provider search results, to surface warnings before a member commits to a location, and to build user experiences that reflect the actual reliability of the underlying data. See the IdeonSelect provider data dictionary for the full field-level specification.
Cost and quality data: accuracy beyond network participation
Accurate provider data has historically meant one thing: knowing whether a provider is in-network. That question matters, but it is increasingly insufficient for the tools that platforms are trying to build.
IdeonSelect now includes provider cost and quality ratings alongside network participation data. This means that a care navigation platform can surface not just whether a specialist is in-network, but how their outcomes compare to peers in the same specialty and geography, and what care from them typically costs relative to alternatives.
The accuracy commitment extends to this data as well. Cost and quality ratings are sourced, validated, and delivered through the same pipeline as network participation data — so platforms can build confident, differentiated experiences without having to source and normalize quality data from a separate provider.
What this means for platforms that build on Ideon
If you are building a healthcare navigation tool, a plan shopping experience, a network analytics platform, or any other product that depends on knowing which providers participate in which plans — the quality of your user experience is a direct function of the quality of your data.
The platforms that trust Ideon's provider data — including Amino Health, Garner Health, Embold, and Healthcare Bluebook, among others — do so because they have tested the alternative. Managing provider data in-house, or accepting carrier data without independent validation, is a costly and ongoing problem. Offloading that problem to a partner that has built its entire process around getting it right is a structural advantage.
Accurate provider network data doesn't happen by accident. It happens through a defined process, a meaningful quality bar, and a commitment to human oversight at every run. That's what we've built — and what every API call to IdeonSelect delivers.
Frequently asked questions
Why is provider network data accuracy so difficult to maintain?
Provider data is not static. Physicians join and leave networks, clinics change addresses, and group practices add and drop insurance contracts continuously. Because additions tend to outpace removals in carrier directories, stale records accumulate over time — creating directories with providers who no longer accept a given plan, at addresses that no longer exist.
What is Ideon's six-stage provider data pipeline?
Ideon processes every provider record through six stages before it reaches the API: Acquire (ingest from 300+ carriers), Validate (structural and integrity checks), Map (normalize to a canonical schema), Auto-QA (automated anomaly detection), Human Review (an analyst reviews every single run with zero unresolved flags allowed), and Deliver (data is promoted to production only after clearing all prior stages). See the full provider data dictionary for field-level detail.
What is an Address Confidence Score?
Ideon's Address Confidence Score is an AI-driven rating (High, Medium, or Low) assigned to every provider address in the IdeonSelect dataset. The model draws on multiple data sources and pattern analysis to assess address reliability — giving platforms the ability to filter or flag low-confidence addresses in provider search results rather than treating all records as equally trustworthy.
Does IdeonSelect include provider cost and quality data?
Yes. IdeonSelect includes provider cost and quality ratings alongside network participation data, sourced and validated through the same pipeline. This enables care navigation platforms to surface provider outcomes and cost comparisons alongside in-network status — without sourcing and normalizing quality data from a separate vendor.
How does Ideon's approach differ from other provider data vendors?
Most vendors ingest carrier-provided data and pass it downstream, treating accuracy as a carrier responsibility. Ideon treats data quality as an active, platform-level responsibility — validating, normalizing, running automated QA, and requiring human analyst sign-off on every single data run. The standard is zero unresolved flags, every run, no exceptions.
See how IdeonSelect's provider data quality holds up
Talk to our team about a data comparison or proof of concept. We'll show you exactly where our data stands against your current source.
Learn about IdeonSelect →